Expert urticaria Treatment
Advanced diagnosis and treatment for your hives, swelling (angioedema), and intense itching
Why do I have these really itchy hives?

The sudden appearance of hives, intense itching, or swelling (angioedema) can cause significant distress.
The worst part isn’t just the itching, but not knowing the cause and the fear that it will happen again or that your throat will swell up. In the emergency room or at the general practitioner’s office, they usually prescribe corticosteroids to quickly ‘put out the fire,’ but they rarely explain the underlying cause.
My goal in the consultation is twofold:
To eliminate the itching AS SOON AS POSSIBLE: To adjust your medication (antihistamines and others) so you can sleep and resume your normal life from day one, without depending on corticosteroids long-term.
To explain the WHY: To analyze whether there is an allergic, infectious, or autoimmune cause. Understanding your condition is the first step to overcoming your fear.
Expert Urticaria Treatment
Why Is Your Current Treatment Not Working? 5 Key Medical Factors
If your current treatment does not achieve complete symptom control, or if you require corticosteroids to manage it, your treatment needs a thorough review based on international guidelines (EAACI). In my practice, we apply this specific protocol.
Furthermore, if you do not understand the causes and mechanisms of your disease—and therefore the treatment—you require an explanation of the underlying mechanisms of urticaria.
Urticaria is a disease characterized by wheals (hives) and redness of the skin, usually accompanied by itching (pruritus). Typically, the lesions disappear or move to a different location within 24 hours. These lesions are typically circular—though they may adopt other shapes due to the coalescence of such circles—and blanch (turn white) upon pressure. Furthermore, these lesions leave no permanent marks on the skin.
1.- The Danger of Oral Corticosteroids:
Repeated use of systemic corticosteroids may control your urticaria, but at the cost of undesirable side effects that we must strive to control as much as possible.
2.- Optimized Antihistamine Dosage:
It is a common error to maintain the standard label dose. Guidelines allow quadrupling the dose of modern antihistamines but only under the supervision of your allergist. The specialist must also assist in selecting the specific antihistamine from the available alternatives, always individualizing the choice based on each patient’s characteristics and minimizing adverse effects such as drowsiness, dizziness, dry mouth, blurred vision, or constipation.
3.- It Is Rarely a Food Allergy:
With the “AI boom” and social media, many patients believe their urticaria is due to food allergies or intolerances and attend consultations having adopted unnecessary restrictive diets and an unjustified fear of eating, creating a vicious circle of unnecessary stress. It is crucial to perform a correct diagnosis, as many cases are due to autoimmune or infectious causes. We need to improve quality of life, not worsen it.
4.- Access to Biological Therapies:
For cases that do not respond to high-dose antihistamines, I will manage access to biological treatments. If these are not immediately available, I will temporarily initiate immunomodulators that block the cells involved in your urticaria.
5.- Rigorous Differential Diagnosis:
It is vital to rule out, through skin tests, provocation tests, or blood work, the different pathologies that can produce urticaria. It is important to note that, in some cases, these include infectious or autoinflammatory diseases such as urticarial vasculitis, which require completely different treatments.
The aim of this article is to explain acute and chronic urticaria in a simple and understandable way for those patients who arrive with the typical complaint: “Doctor, I have hives and they won’t go away.”
In patients where the disease develops in the mucous membranes instead of the skin, swelling known as angioedema occurs. Urticaria and angioedema are part of the same disease spectrum and, therefore, frequently occur simultaneously.
Urticaria is a disease that only in very isolated cases can lead to patient death; these cases are practically limited to severe reactions to drugs, foods, insect stings, or patients presenting with angioedema of the airways. Urticaria significantly alters the patient’s quality of life given the constant itching, which prevents a normal life, affecting work, leisure, study, or any other daily activity. The ideal urticaria treatment is one that restores optimal quality of life to the patient.
A very common phrase at the start of a consultation is: “I have urticaria that won’t go away.” It is the allergist’s job to ensure the patient leads an absolutely normal life without depending on drugs with side effects, such as oral corticosteroids. For effective urticaria treatment, it is important to monitor the side effects of antihistamines.
If you are reading this article, you may be aware of how unbearable this disease is, both for the patient and the doctor, as it is rarely solved in the first visit. An example identifying this doctor-patient bond is the poetry by Spanish doctor Ignacio Dávila.
- Expert urticaria Treatment
- Why do I have these really itchy hives?
- Expert Urticaria Treatment
- Why Is Your Current Treatment Not Working? 5 Key Medical Factors
- Dr. Tito Rodriguez Bouza
- Keys to Effective and Lasting Treatment
- What is the medical treatment for Urticaria?
- Let's talk? Stop treating just the symptoms. Let's find the cause.
- Expert Urticaria Treatment
What is the mechanism behind wheals and itching?
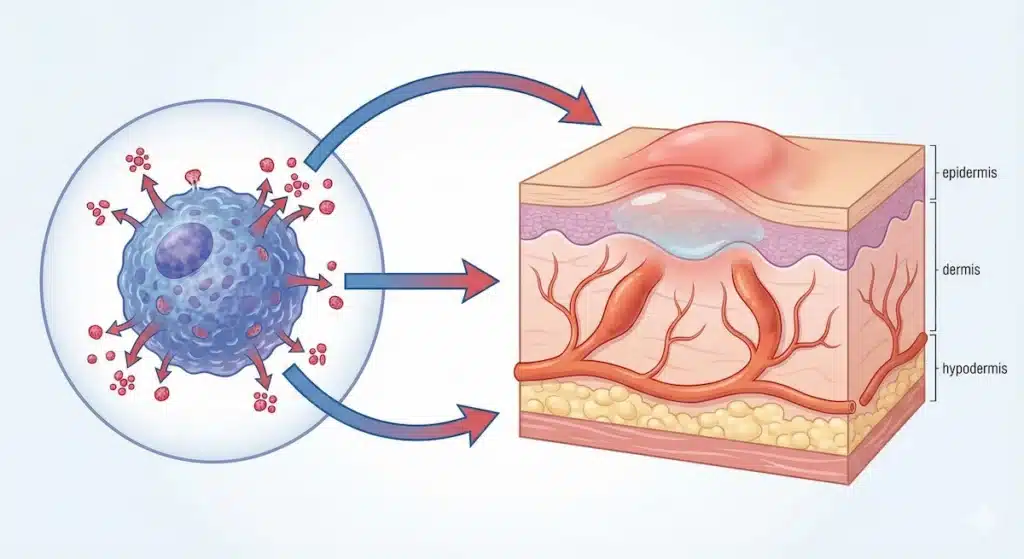
Urticaria is caused by the activation of cells found in our skin called mast cells. These cells release a protein called histamine.
Histamine activates itch (pruritus) receptors and causes blood vessels to enlarge and dilate, creating a pooling of blood (hence the red color of the skin lesions). Since these blood vessels have tiny gaps, dilation allows fluid without red blood cells to escape, causing the pale swelling or “wheal” on the skin.
It is important to note that not all patients produce the same amount of histamine; therefore, antihistamine treatment must not be the same for every patient. The activation of these mast cells also triggers the recruitment of other cell types to the inflamed skin area—a phenomenon that occurs in other allergic diseases—although this cellular accumulation in the skin causes fewer problems for the patient than the same process occurring, for example, in the nose during allergic rhinitis.
Mast cells can also be inhibited with oral corticosteroids, but antihistamines are the initial option given their low side-effect profile compared to oral corticosteroids.
Types of Urticaria: Chronic and Acute
It is crucial for the allergist to determine if the urticaria has lasted more or less than 6 weeks, as we classify it as acute or chronic based on this duration. The differences between the two are explained below:
Chronic Urticaria: when it lasts more than 6 weeks.
Chronic spontaneous urticaria (CSU), unlike acute urticaria, is not caused by an identifiable external trigger, although there are circumstances that can reactivate it, often confusing patients who believe this trigger is the cause of the disease.
It is important to know that this disease disappears spontaneously in 65% of cases after 3 years and in 85% after 5 years, with approximately 2% of cases persisting for more than 10 years. The allergist can provide an estimate of how many years the urticaria may persist, but the patient must understand that this calculation is not precise.
Currently, we have increasing scientific evidence that chronic spontaneous urticaria appears to be produced by an autoimmune mechanism, or in other words, our own defense system attacking our body’s cells by mistake.
An example of this association is that this disease is closely related to autoimmune thyroid disease, where our own body attacks the thyroid gland, causing hypothyroidism and urticaria.
In patients with chronic spontaneous urticaria, the allergist must perform at least one blood test, as CSU can be related to other diseases that may be more serious than the urticaria itself.
The allergist must reasonably rule out the presence of such diseases. The specific blood work will depend on each patient’s characteristics but can generally be performed in any laboratory, as it does not require great complexity.
Acute Urticaria: when it lasts less than 6 weeks.
It tends to occur as a rapid consequence (less than 2 hours) of some type of stimulus.
Stimuli that can cause acute urticaria include viral infections, allergic reactions to antibiotics and other medicines, insect bites, physical stimuli such as cold, pressure, or sun, and a wide range of other substances.
It is the allergist’s job to take an adequate clinical history (a proper interview) of the patient who arrives stating “I have hives that won’t go away,” asking about all stimuli that could provoke acute urticaria. In my personal experience, patients tend to misinterpret such stimuli, leading many to believe their symptoms are caused by food when it is not the culprit of their disease.
Dr. Tito Rodriguez Bouza
“My approach is based on precision medicine, combining clinical practice with deep knowledge of disease mechanisms acquired during my 3 years as a researcher at Brigham and Women’s Hospital (Harvard Medical School).
This experience allows me not only to protocolize the treatment of resistant urticaria but also to explain to you—with the depth you require—why your pathology occurs.
My goal is to stop the medical pilgrimage caused by ineffective treatments or a lack of clear explanations. We treat both acute and chronic urticaria by modulating the immune response, not just the skin.”
Keys to Effective and Lasting Treatment
The first thing to remember is that this disease is usually desperate for the patient, who suffers excessively during the wait required for the allergist to adjust the treatment until a normal life without itching is achieved. This is usually achieved in one, two, or three follow-up visits. The recurrent patient has “hives that won’t go away”; therefore, trust in their allergist is required. We will try to find the key in the first consultation, but occasionally adjustments over several visits are needed to obtain effective urticaria treatment.
In the vast majority of cases, we can control it with different doses and combinations of antihistamines. However, in a minority of cases—precisely those who come saying “I have hives that won’t go away”—modern drugs called monoclonal antibodies will be needed. Dr. Tito Rodríguez Bouza has proven experience with these, or alternatives such as cyclosporine, among other types of drugs. These advanced drugs require the advice of an allergist and have a better safety profile than oral corticosteroids.
Since it is a recurring error, if you have been prescribed oral corticosteroids, I must mention that there are many other treatment options. Corticosteroids should be reserved for urgent severe cases but never for the long term, as they present a high number of undesirable side effects. Oral corticosteroids are used in emergency departments, but they cannot be the treatment of choice for the long term. I have written an article about this, given how recurrent this problem is when trying to achieve effective urticaria treatment.
What is the medical treatment for Urticaria?
There is no single treatment that works for all patients. Each patient must be individualized based primarily on symptom severity, potential side effects, other existing diseases, and the failure of previous treatments. Furthermore, in general terms, guidelines speak of “therapeutic steps,” which are essentially a scale of increasing potency (usually implying side effects or increased cost) that must be followed individually for each patient.
These therapeutic steps include, among others:
- Non-sedating antihistamines (licensed and high doses): New second-generation antihistamines cause less drowsiness and are very safe for urticaria treatment. In urticaria, standard label doses are often insufficient. International guidelines recommend increasing the dose up to four times (quadruple dose) under medical supervision before considering treatment failure. The choice must be individualized according to each patient and their characteristics.
- Oral Corticosteroids: Although overused by emergency departments in general, they should only be used to “put out the fire” in severe acute crises, under the control of your allergist, to reduce usage time. Their short-term use, but especially when prolonged, is associated with side effects such as weight gain, hypertension, growth reduction, or bone damage, among others.
- Immunomodulators: Reserved for severe and resistant cases. They can be used as an alternative to corticosteroids for urticaria treatment, always under strict medical supervision due to their potential side effects.
- Antileukotrienes (for selected cases): Useful mainly in delayed pressure urticaria.
- Biological drugs (high cost): For Chronic Spontaneous Urticaria (CSU) that does not respond to high doses of antihistamines, the use of monoclonal antibodies has revolutionized treatment. It is an injectable drug for hospital or home use that is very safe and effective in a high percentage of patients. It can only be administered under strict criteria and after therapeutic escalation.
Why request an online consultation?
If you have hives that won’t go away, an online video consultation is especially indicated for you. This is due to the ease of quickly contacting your allergist and, therefore, making the two or three medication changes usually required to control the patient. To achieve effective urticaria treatment, follow-up and specialist consultations will be necessary.
In a traditional consultation, this can be delayed for weeks or months, unnecessarily prolonging the patient’s suffering and itching. On the other hand, since tests other than blood work are generally not required, diagnosis can be performed simply, as the doctor can request blood tests to be done at the patient’s laboratory of convenience.
Furthermore, given the patient’s suffering, it is advisable to find a true specialist in the field to reduce it. The only limitation of online consultation would be for those few patients where disease control is not achieved after two or three reviews, and treatments that can only be administered in a hospital setting are necessary to achieve total disease control.
It should be noted, however, that even in these patients, online urticaria consultation can help temporarily adjust treatments until definitive treatment is established, always avoiding the long-term use of oral corticosteroids.
But how will you do allergy tests or prescriptions?
In Allergology, there are tests performed in person in the allergy clinic (skin prick tests, patches, spirometry) and non-face-to-face tests or tests performed by other practitioners (blood tests, cytology, provocation tests, FeNO, etc.).
In cases of urticaria, with rare exceptions, skin tests, patches, or spirometry are not indicated. Instead, generally, what is required are blood tests that can be conveniently performed near your place of residence without having to travel to the clinic. To achieve effective online urticaria treatment, prescriptions can be issued throughout Europe or via other mechanisms in other countries, depending on the location.
If you have been seen in an emergency department, it is worth noting that it causes great confusion that many ER doctors continue to say—purely out of tradition—”go to an allergist to get allergy tests done,” just as they continue to prescribe old drugs or give dietary recommendations that have been abandoned by allergists years ago due to lack of scientific evidence. ER doctors, ultimately, are not specialists in this field and can make mistakes, just as I would if I had to opine, for example, on a neurology case.
Even so, if after reading this you prefer a face-to-face consultation, the reality is that, in total numbers as of 2024, patients still prefer face-to-face over online consultations. Therefore, I am the first to recommend a face-to-face consultation if you are not comfortable with the online format. I encourage you, however, to try this modality and ensure it is by video conference and not by phone.
Curiously, at the time of writing this article, there are still no studies comparing patient preferences when approaching urticaria treatment, nor studies comparing the effectiveness of obtaining effective treatment in online vs. face-to-face consultations.
Dermatologist or Allergist: Who should treat your urticaria?
In reality, urticaria is a disease that both specialists can initially treat in the same way. After a first consultation, some cases of urticaria, such as urticarial vasculitis among others, should be referred to a dermatologist for treatment. Likewise, some cases where allergic pathology is suspected must be referred to your allergist for effective urticaria treatment.
Therefore, the answer is that whether you have been referred to an allergist or a dermatologist, effective urticaria treatment can be achieved in both cases, and thus, the correct decision has been made in either case.
Let’s talk? Stop treating just the symptoms. Let’s find the cause.
- In-Person (Madrid) and Online Consultation.
- Private Fee: €150 | Insurers: Adeslas and Nueva Mutua
Expert Urticaria Treatment

Hi I’ve been suffering from this hives thing since March 2021 till now…I’ve been on different meds and still it surfaces. I dont know what to do.
Good evening and apologies for my very late reply. Please let me know to my whatsapp or contact from ( https://www.drtitorodriguezbouza.com/contact-en/ ) and I could absolutely help on this matter.
Itchy rednessurcicaria colds
Yes, i can help on that one via consultation if interested
i have this hives since 2019..not itchy before and the color is the color of my skin..located in my neck . before its very little but now its all over my neck and getting itchy..
I can help in this case